

Yves right here. This examine seems to be at an essential matter: what causes inequality of well being by revenue strata? It’s widely known that richer individuals typically have higher well being than poorer individuals, however how does that come about? This information comes from Denmark, which has an excellent well being system that provides top quality care to decrease revenue teams. The massive findings are that poorer individuals undergo from continual illnesses at a better stage and youthful than the extra prosperous. This isn’t primarily attributable to a care hole. As soon as a situation is recognized, the outcomes are comparable by revenue group. Nevertheless, the authors level out that situations could also be recognized later among the many much less effectively off, so they could have been spared having a continual situation if there was higher preventative care.
The article doesn’t unpack the diploma to which environmental components, like dwelling in areas that may straight impair well being (poor air high quality through dwelling close to huge site visitors arteries, extra publicity to toxins through dwelling close to chemical crops) or in jobs that may hurt well being contributed to the well being differential. Readers can inform me the diploma to which decrease revenue Danes would possibly wind up consuming much less wholesome meals, which within the US is an enormous contributor to weight problems.
After all, the causality runs the opposite approach too: that these with continual situations may discover it tougher to wind up on a better revenue observe.
By Kaveh Danesh, Inner medication resident College of California, San Francisco, Jonathan Kolstad, Affiliate Professor, Haas College of Enterprise College of California, Berkeley, William Parker, PhD candidate London College Of Economics And Political Science, and Johannes Spinnewijn, Professor in Economics London College Of Economics And Political Science. Initially revealed at VoxEU
Although well being disparities have lengthy been the topic of analysis and debate, life expectancy gaps between wealthy and poor stay placing, even in international locations with common entry to healthcare. This column analyses the roots of well being inequality utilizing information from the Netherlands. Whereas mortality variations are most obvious at old-age, continual sickness begins shaping these inequalities a lot earlier in life than generally recognised. Socioeconomic standing and geographic disparities play a essential position in continual illness improvement, surpassing the influence of unhealthy behaviours comparable to smoking and ingesting.
Within the Netherlands, healthcare entry is roughly common, with simply 0.4% of poor households reporting unmet medical wants (Eurostat 2023). Nevertheless, inequality of life expectancy stays pronounced: throughout the family revenue distribution, the hole is 7.6 years for ladies and 11.6 years for males. That is per figures elsewhere in Europe, and little higher than outcomes from the US (Chetty et al. 2016, Schwandt et al. 2021, Currie and Schwandt 2016, Bohacek et al. 2018).
Regardless of the significance of the problem and the eye paid in coverage and analysis, the complexity of the well being manufacturing perform together with measurement challenges have restricted our understanding of what drives well being inequality. As Angus Deaton has noticed: “there isn’t a common settlement about its causes … and what obvious settlement there may be, is typically higher supported by repeated assertion than by stable proof” (Deaton 2002).
Our new analysis (Danesh et al. 2024) focuses on continual sickness to review how well being inequalities develop over the lifecycle. Continual sickness isn’t solely a key contributor to the mortality-income gradient, but in addition a measurable, dynamic marker of inhabitants well being (Bloom 2022). As such, it permits us to trace a key measure of well being that contributes to mortality gaps in older age, lengthy earlier than these mortality results manifest themselves. Constructing on prior work (e.g. Huber et al. 2013), we use distributed treatment to establish continual situations. These information can be found on the particular person stage for your entire Dutch inhabitants since 2006. We straight handle considerations relating to unequal underdiagnosis and/or insufficient administration of continual situations, utilizing further info from survey information and different medication use. We discover that detection and drugs charges are constant throughout the revenue distribution, apart from the very backside 5%–10%.
Determine 1 plots the prevalence of all continual illnesses at old-age and highlights their greater prevalence for people with below-median family revenue. We separate out the underside 10% (D1), illustrating the decrease prevalence of some situations (e.g. heart problems) for this group, probably attributable to under-diagnosis and/or administration. General, we discover that differential prevalence of continual situations can clarify 30–40% of the hole in old-age mortality between low- and high-income teams. Furthermore, we don’t discover significant variations in mortality conditional on continual illness, suggesting that people recognized with a given continual situation obtain therapy of comparable high quality no matter their revenue group. That is additional corroborated by comparable healthcare expenditures conditional on continual situations throughout the revenue distribution.
Determine 1 Variations in continual illness prevalence by revenue at age 70
Dynamic Forces Behind the Mortality Hole
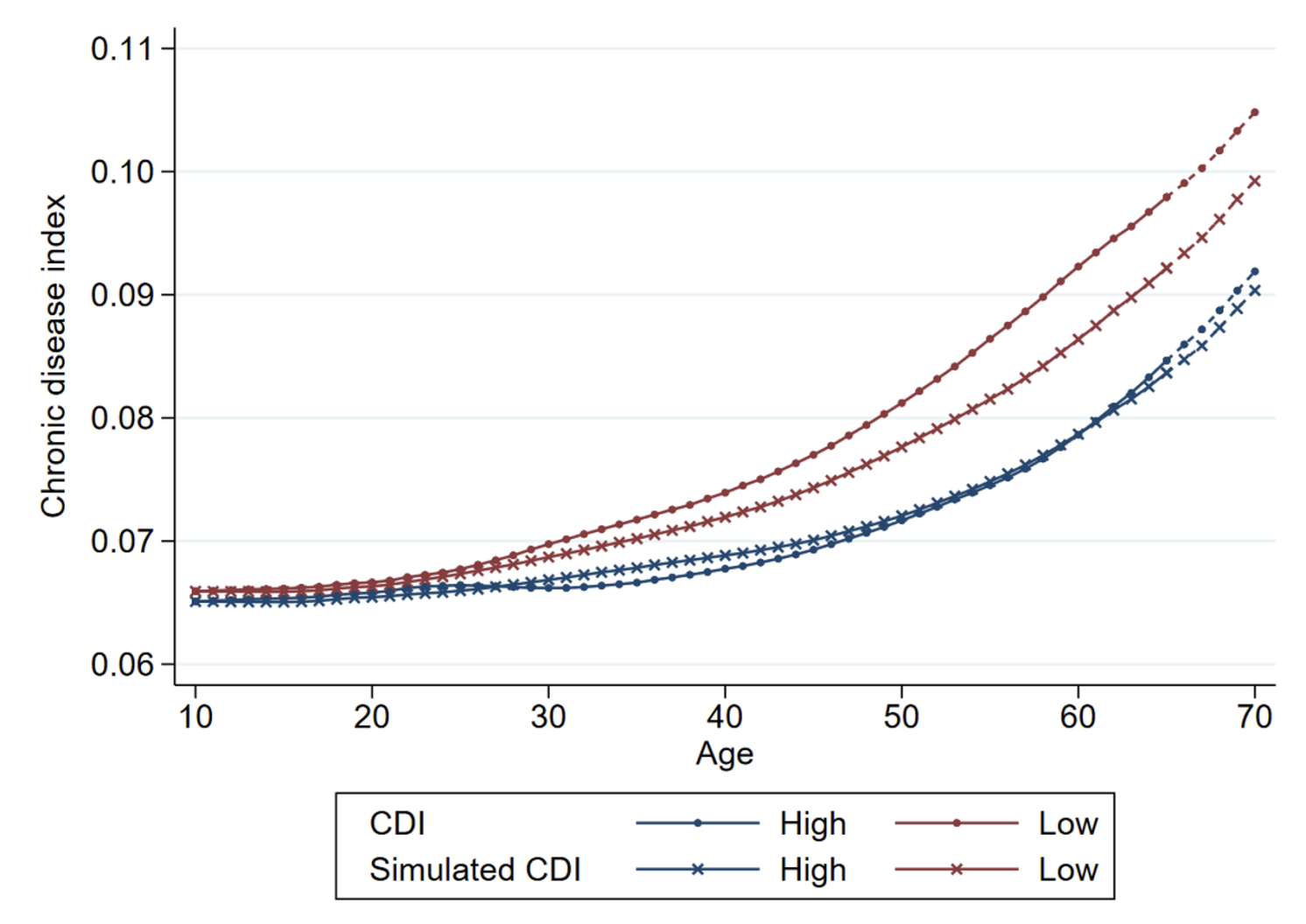
Whereas gaps in mortality danger are most obvious post-retirement age, our evaluation reveals these forces are effectively established earlier in life. We assemble a Continual Illness Index (CDI) for all people and in any respect ages, capturing how their point-in-time continual situations would collectively predict mortality danger at old-age. Determine 2 visualises how the typical CDI evolves over the lifecycle, for low- and high-income people individually. The dynamic collection reveals that half of the measured hole at age 70 has already materialised at age 40, indicating the necessity for early interventions to shut the well being hole.
Two major forces drive the rise within the well being hole with age: differential ageing, whereby low-income people develop continual sickness at a quicker price; and health-based sorting, whereby chronically ailing people type into low-income teams. Determine 2 additionally reveals the simulated CDI excluding the health-based sorting impact, and highlights that extra fast ageing amongst low-income people happens in early maturity. Although each forces are vital, our estimates point out that differential ageing is the dominant issue: it contributes 40% greater than health-based sorting to the hole in continual illness burden at age 70.
This underscores how people in several revenue teams expertise distinctive well being trajectories, and the necessity for interventions to take care of the social determinants of well being at an earlier age. Specializing in the position of single continual situations, we discover that the differential incidence of heart problems, diabetes, and respiratory illness contribute most to differential ageing all through maturity. We additionally see substantial variations within the prevalence of psychological issues contributing most to the hole in CDI ranges already at younger ages.
Determine 2 The well being hole over the life cycle
Mediators of Continual Illness
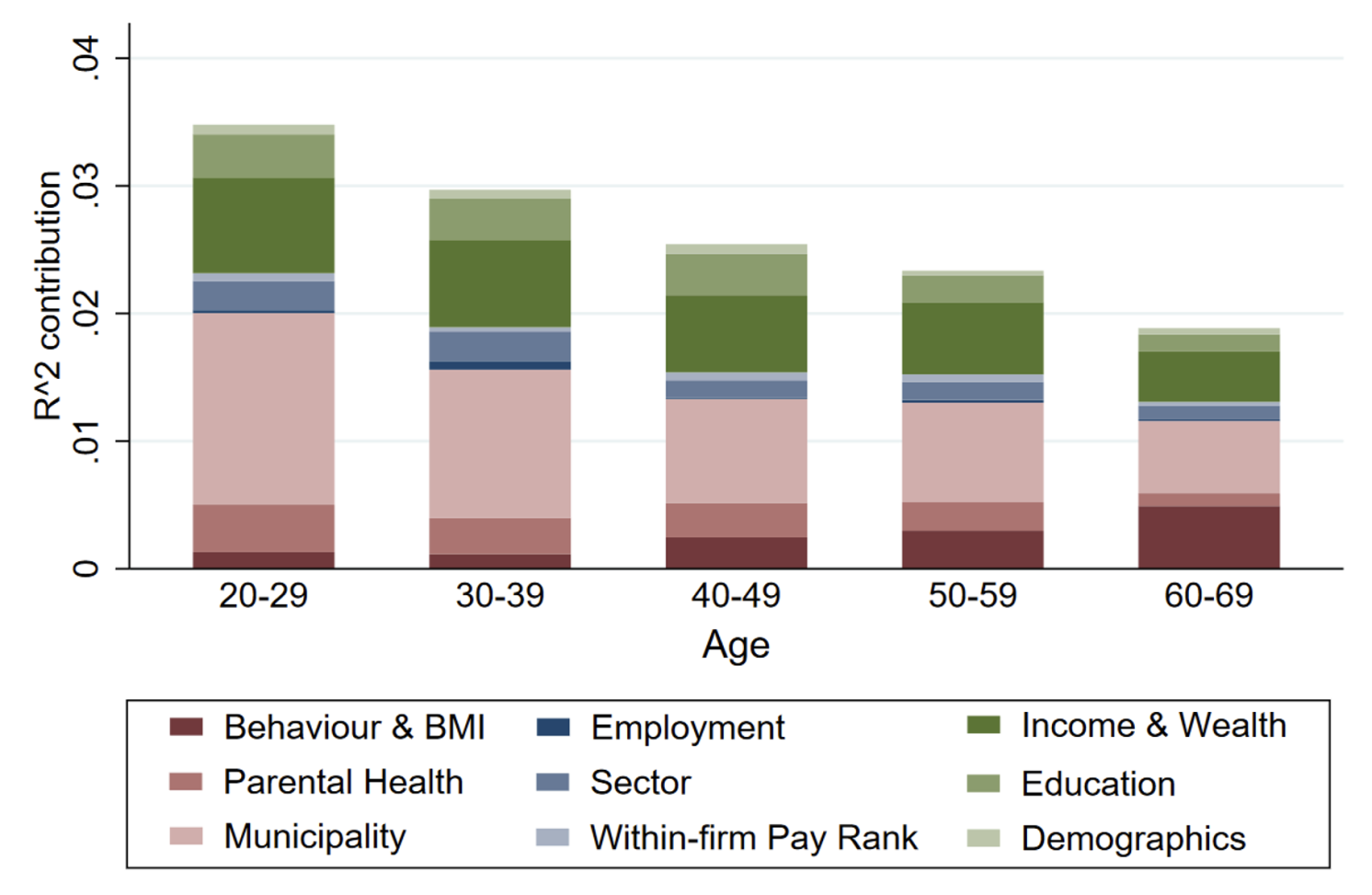
Having established the distinction in well being trajectories, we will additionally make clear the related components mediating these trajectories. We leverage the wealthy information atmosphere within the Netherlands, which incorporates not solely numerous administrative registers, but in addition linked survey information. In distinction with prior work, we will account for a spread of mediating components collectively in the identical context, and thus present a complete account of their relative significance. Utilizing Shapley-Owen decompositions, which apportion the generally defined variation by totally different mediators, we discover that socioeconomic standing and geography contribute most to the defined variation within the incidence of continual situations, accounting for about one third every. Determine 3 illustrates these findings. In distinction, we discover a much less essential position for noticed well being behaviours (i.e. smoking, ingesting, train, physique mass index) and occupational components (e.g. sector of labor, within-firm pay rank).
Whereas this evaluation is descriptive, it supplies an essential recalibration of the potential significance of various determinants of well being, as prior work emphasised particular person well being behaviours as the important thing driving issue (e.g. McGinnis et al. 2002). Apparently, the richness of the information permits us for instance the potential for misestimation attributable to information challenges. Particularly, we present {that a} extra partial evaluation (e.g. not controlling for different social and geographic components) or the failure to account for reverse causalities (e.g. learning prevalence moderately than incidence) would overestimate the significance of generally measured well being behaviours.
Determine 3 Relative significance of mediators for five-year development in CDI
Conclusions and Coverage Implications
In lots of international locations, healthcare spending is directed virtually completely in the direction of therapy, regardless of the excessive returns to prevention. By exhibiting their potential to cut back the well being hole, our evaluation strengthens the case for investments in preventive insurance policies. Particularly, our analysis demonstrates that variations within the incidence of poor well being situations are a extra vital driver of well being disparities than variations in therapy. Furthermore, we discover that well being inequality begins a lot earlier in life than historically recognised, with vital disparities already obvious at center age. The first driver is differential ageing throughout the revenue spectrum, to the detriment of low-income individuals. Addressing this disparity early in life is crucial for lowering well being inequality.
Efficient coverage ought to concentrate on interventions focusing on the early-life determinants of well being, and transfer past the present concentrate on unhealthy behaviours comparable to smoking and ingesting. Particularly, socioeconomic standing and geographic disparities play a essential position in continual illness improvement, surpassing the influence of particular person well being behaviours. Complete methods that handle these components earlier than they translate into continual illness are important to making a extra equitable well being panorama.
See authentic submit for references







/cdn.vox-cdn.com/uploads/chorus_asset/file/25636593/pinterest_collage.jpg "Pinterest’s new remix feature can jump-start your mood board")




")

{kind=link}